
Discussion: Caregivers
As health educators, we must continuously develop strategies to overcome barriers and challenges faced by elders and their caregivers. What specific barriers do you identify that impact these people?

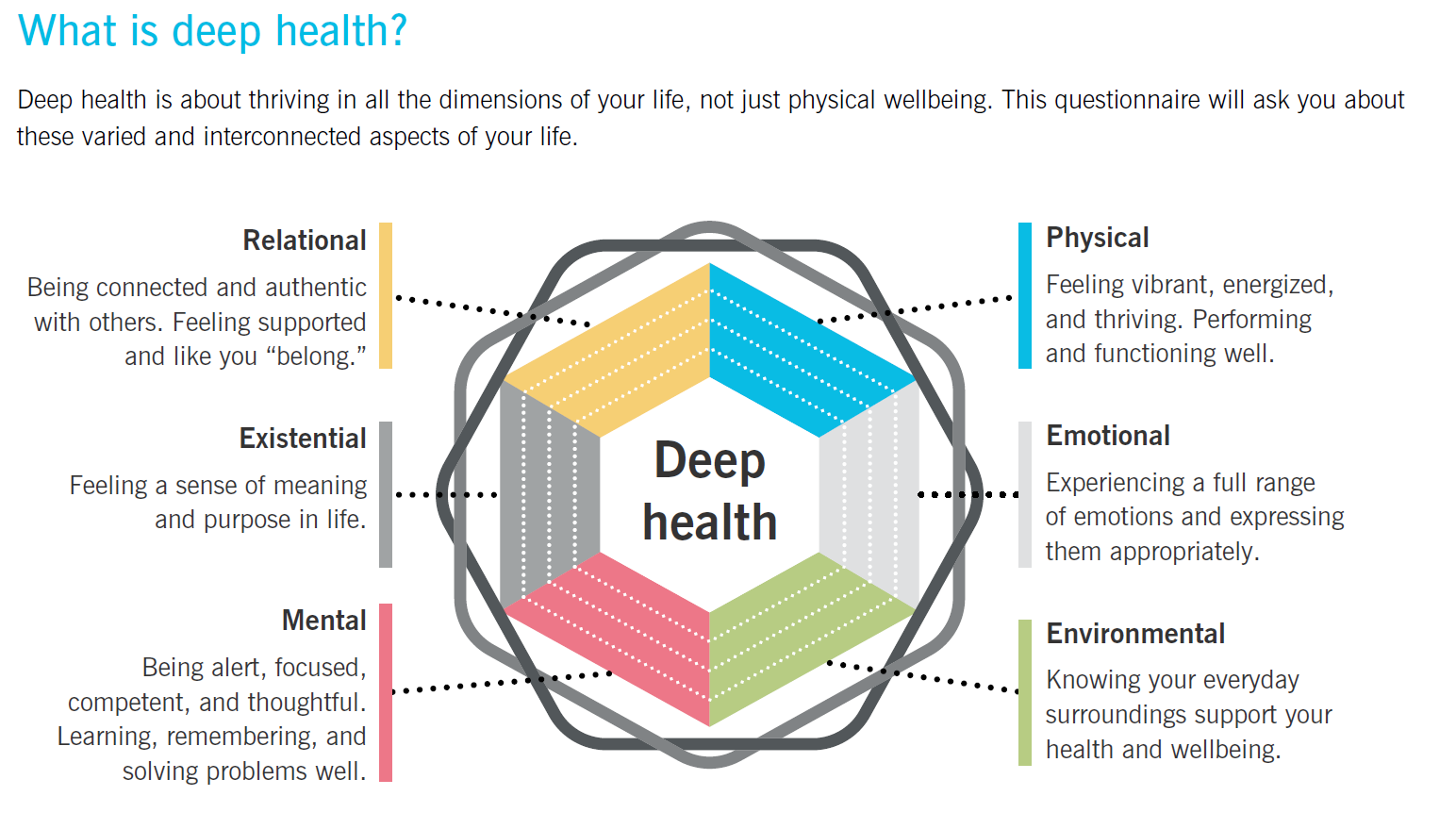
When discussing the barriers that impact elders and their caregivers, we can qualify them under the Six Dimensions of Health, as listed by Precision Nutrition (n.d.):
Physical
Mental
Emotional
Relational
Environmental
Existential
The barriers associated with physical health are biological in nature and include the progressive wear and tear from a lifetime of cellular mitosis and mitochondrial degradation (Perez, 2026a; van der Rijt et al., 2020). This progressive decline also includes the decrease in hormone production and physiological efficiency, which makes it challenging for the body to maintain allostasis (Pfaltz & Schnyder, 2023). As is highlighted in the Dynamic Flourishing Hierarchy (DFH), “the deliberate, systemic provision of biological and psychological safety required to reduce chronic physiological wear and tear” is an essential component for supporting self-sovereignty and securing the Integrated Survival Bedrock (Perez, 2026b). This aligns with the clinical understanding of allostatic load, which is defined as “the strain on the body produced by systems under challenge and the changes in metabolism and wear and tear on a number of organs and tissues” (Pfaltz & Schnyder, 2023). This degradation of the physical vessel can manifest not only through decreases in physical mobility and capacity, but also through cognitive (mental), emotional, and existential challenges, which can also affect relational health (Overstreet, n.d.; Precision Nutrition, n.d.; Touro University Worldwide, n.d.). Vaziri et al. (2020) cite physical inactivity as a “major risk factor for chronic diseases, early mortality and increasing healthcare costs.”
Mental health requires “being alert, focused, competent, and thoughtful. Learning, remembering, and solving problems well”, whereas emotional and existential health are associated with “experiencing a full range of emotions and expressing them appropriately,” as well as “feeling a sense of meaning and purpose in life” (Precision Nutrition, n.d.). I personally feel that all of these are so closely tied in because (as previously discussed) the barriers associated with cognitive (mental), emotional, and existential health can be issues that are rooted in biological degradation and changes, such as dementia and Alzheimer’s disease (Overstreet, n.d.). In 2009 alone, an estimated 5.3 million people in the United States were afflicted with Alzheimer’s disease, a degenerative form of dementia” (Lykens et al., 2014). Psychosocial and environmental factors can also be the root factors for cognitive health struggles such as poverty, social distancing regulations that lead to increased isolation or increased isolation for other reasons, and even ruminations on lives that are perceived as unfulfilled or unproductive, which lead to despair, depression, and hopelessness (Mastrogiovanni et al., 2022, Overstreet, n.d.; Touro University Worldwide, n.d.). It is reminiscent to me of the ouroboros – the untenable cycle of the snake consuming itself; one’s physical decline leading to cognitive decline, which leads to emotional distress, which leads to existential dread and crisis, all exacerbated by increasing demands on relational health.
Relational health requires “being connected and authentic with others,” as well as “feeling supported and like you ‘belong’” (Precision Nutrition, n.d.). However, elders face significant systemic and environmental barriers to maintaining these connections. For example, recent years have shown how global events and “social distancing regulations have led to an increased risk of social isolation and physical inactivity, particularly among older adults” (Mastrogiovanni et al., 2022. From a biological standpoint, this loss of social connection is devastating. As outlined in the Dynamic Flourishing Hierarchy (DFH), “Load Sharing occurs as the brain literally incorporates relational partners into its neural representations of the self” and an individual’s cognitive and emotional resources are conserved when they have others to rely on (Perez, 2026b). When older adults face physical and cognitive decline, and simultaneously lose their peer networks, their environmental demands increase while their load-sharing partners decrease. This leads to an immense biological and logistical burden shift that may directly impact family and/or caregivers. When dealing with severe cognitive decline, “the impact of this disease is not limited to the patient but also has significant impact on the lives and health of their family caregivers” (Lykens et al., 2014). The barriers these caregivers face are often systemic and disproportionate; “caregiving responsibilities continue to fall primarily to women and some subgroups at greater risk for negative consequences – including caregivers to persons with dementia and those who have limited financial resources” (Johns Hopkins Bloomberg School of Public Health, 2025). As a result, “caregiver role strain is a common issue as the intensity and duration of care required escalate” (Touro University Worldwide, n.d.). Caregivers frequently sacrifice their own biological necessities, facing internal barriers of guilt and self-neglect (and as a mother and caregiver in my own right, I can vouch for this reality).
As DiLonardo (2024) notes, “When you’re caring for someone else, it’s often hard to focus on your own needs. You may even feel guilty when you do.” Ultimately, if these environmental demands exceed the caregiver’s resources, their physiological systems dysregulate, resulting in allostatic overload, which manifests as “sleep disturbances, irritability, impaired social or occupational functioning, and feelings of being overwhelmed” (Pfaltz & Schnyder, 2023). The ouroboros of issues and barriers rears its ugly head again, as the barriers affecting the elderly also become the barriers affecting the caregivers.
To break this untenable ouroboros of compounding barriers, we must fundamentally restructure how we approach the aging process and caregiver support. As proposed in the Dynamic Flourishing Hierarchy (DFH), true optimization cannot exist in an isolated dyad of patient and caregiver; rather, it is a “continuous, dynamic pulse of bioenergetic contribution and recovery, inherently dependent upon the structural integrity of both the individual and the collective” (Perez, 2026b). If we are to mitigate the allostatic overload placed on family caregivers, health educators and communities must facilitate environments that provide systemic Allostatic Support for both the caregivers and the elderly, securing their Integrated Survival Bedrock so they do not operate from a space of deficit. Additionally, we must intentionally rebuild the relational networks that older adults lose. By expanding the network of care beyond a single, isolated caregiver and into a broader, reliable social ecology, “the collective effectively frees up the metabolic and cognitive energy of its constituents” (Perez, 2026b). Only by shifting the burden from the exhausted individual to a resilient, interconnected collective can we transform the descent into old age from a crisis of degradation into a stage of supported self-sovereignty.
References
DiLonardo, M. J. (2024, May 15). Caregiving for older adults. WebMD. https://www.webmd.com/healthy-aging/aging-caregiving-older-adults
Johns Hopkins Bloomberg School of Public Health. (2025, February 4). Number of family caregivers supporting older adults increased nearly one-third between 2011 and
2022. https://publichealth.jhu.edu/2025/number-of-family-caregivers-supporting-older-adults-increased-nearly-one-third-between-2011-and-2022
Lykens, K., Moayad, N., Biswas, S., Reyes-Ortiz, C., & Singh, K. P. (2014). Impact of a community based implementation of REACH II program for caregivers of Alzheimer’s
patients. PLoS ONE, 9(2), e89290. https://doi.org/10.1371/journal.pone.0089290
Mastrogiovanni, C., Rosenbaum, S., Delbaere, K., Tiedemann, A., Teasdale, S., McGavin, A., Briggs, N., & McKeon, G. (2022). A mental health-informed, online health
promotion programme targeting physical activity and healthy eating for adults aged 60+ years: Study protocol for the Moving Together randomised controlled trial. Trials,
23, Article 1052. https://doi.org/10.1186/s13063-022-06978-3
Overstreet, L. (n.d.). Introduction to late adulthood. Lumen Learning. https://courses.lumenlearning.com/lifespandevelopment2/chapter/introduction-to-late-adulthood/
Perez, G. (2026a). Discussion 1: The thought process with aging [Discussion board post]. Touro University Worldwide.
https://portal.tuw.edu/
Perez, G. (2026b). The Dynamic Flourishing Hierarchy: A bio-psychological synthesis of individual sovereignty and collective resilience [Unpublished manuscript]. Master of
Science in Health Sciences Program, Touro University.
Pfaltz, M. C., & Schnyder, U. (2023). Allostatic load and allostatic overload: Preventive and clinical implications. Psychotherapy and Psychosomatics, 92(5), 279–282.
https://doi.org/10.1159/000534340
Precision Nutrition. (n.d.). Deep health questionnaire & assessment [PDF document].
Touro University Worldwide. (n.d.). Module 7: Elderly [Lecture notes]. MHS600.
van der Rijt, S., Molenaars, M., McIntyre, R. L., Janssens, G. E., & Houtkooper, R. H. (2020). Integrating the hallmarks of aging throughout the tree of life: A focus on mitochondrial dysfunction. Frontiers in Cell and Developmental Biology, 8, Article 594416. https://doi.org/10.3389/fcell.2020.594416
Vaziri, D. D., Giannouli, E., Frisiello, A., Kaartinen, N., Wieching, R., Schreiber, D., & Wulf, V. (2020). Exploring influencing factors of technology use for active and healthy ageing support in older adults. Behaviour & Information Technology, 39(9), 1011–1021. https://doi.org/10.1080/0144929X.2019.1637457